
When your kidneys fail, dialysis becomes a lifeline. But the real key to surviving dialysis long-term isn’t just the machine-it’s the dialysis access. This is the gateway your blood uses to get cleaned, and not all access types are created equal. Choosing the right one, and caring for it properly, can mean the difference between months of hospital visits and years of stable, independent living.
Why Dialysis Access Matters More Than You Think
Think of dialysis access like a highway for your blood. Every treatment, every week, your blood flows out of your body, gets cleaned by a machine, and flows back. If that highway is narrow, clogged, or infected, your treatments become risky, painful, and less effective. The type of access you have directly affects your risk of infection, hospitalization, and even death.
According to the National Kidney Foundation, patients using central venous catheters have a 1.5 times higher risk of dying compared to those with an arteriovenous (AV) fistula. That’s not a small difference-it’s 84 extra deaths per 100,000 patient-years. And it’s not just about survival. Catheters mean more infections, more missed treatments, and more restrictions on daily life. A fistula, when it works right, can last decades. A graft might last a few years. A catheter? Often, it’s a temporary fix that becomes a long-term burden.
AV Fistula: The Gold Standard
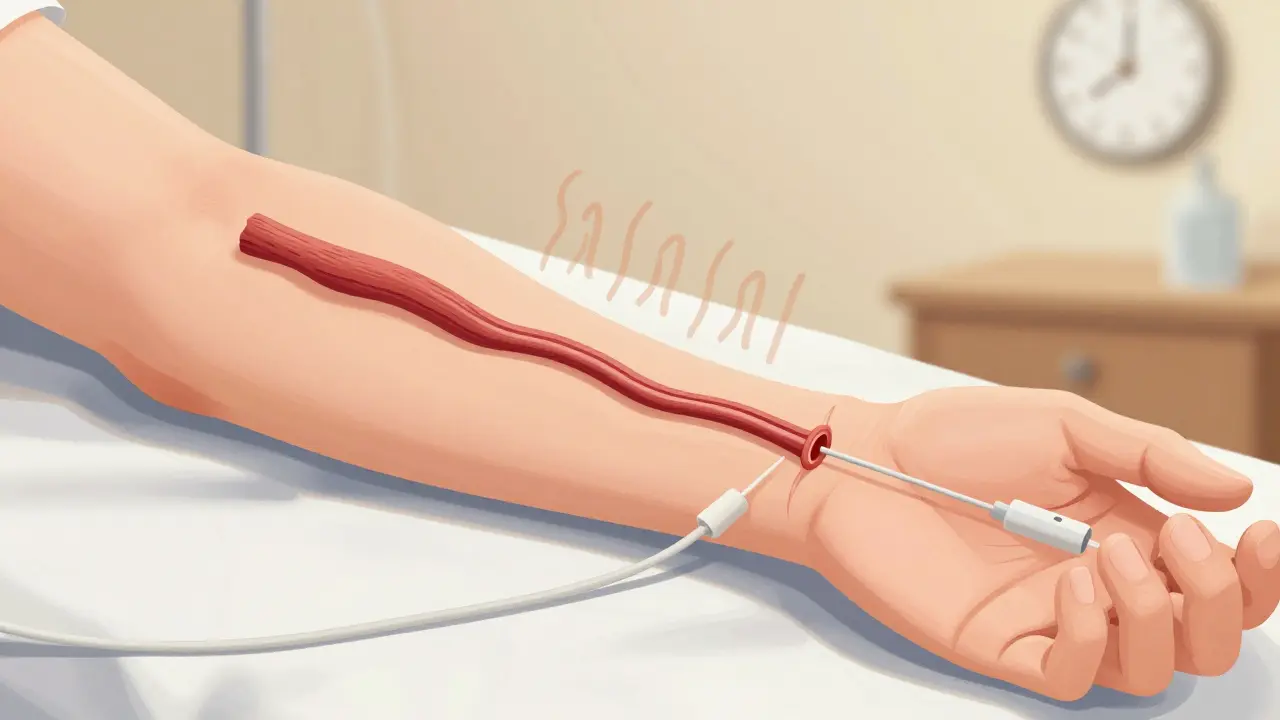
An AV fistula is made by surgically connecting an artery directly to a vein, usually in your forearm. This sounds simple, but the magic happens after surgery. Over 6 to 8 weeks, the vein grows larger and stronger from the high-pressure blood flow from the artery. It becomes thick-walled and bouncy-perfect for repeated needle insertions during dialysis.
This is the most reliable access option. It has the lowest infection rates, the least clotting, and lasts the longest. Many patients use the same fistula for 10, 15, even 20 years. You’ll feel a slight vibration-called a ‘thrill’-when you place your fingers over it. That’s a good sign. No thrill? That could mean a clot or narrowing, and you need to call your care team right away.
But fistulas aren’t perfect. They take time to mature. If you need dialysis urgently, you can’t wait 8 weeks. That’s why some people start with a catheter and switch later. Also, not everyone is a candidate. If your veins are too small, too weak, or blocked by scar tissue from past IVs or high blood pressure, a fistula might not be possible. That’s why vein mapping-a simple ultrasound scan-is done before any surgery. It checks if your vessels can handle the job.
AV Graft: The Backup Plan
If your veins aren’t strong enough for a fistula, an AV graft is the next best thing. Instead of connecting artery to vein directly, a synthetic tube (usually made of PTFE, a type of plastic) is placed between them. This tube is inserted under the skin, usually in the arm, and can be used in just 2 to 3 weeks.
It’s faster than a fistula, but it comes with trade-offs. Grafts clot more often. They’re more prone to infection. Studies show 30 to 50% of grafts need at least one intervention in the first year-sometimes more. That means procedures to open blocked areas, called thrombectomies or angioplasties. These aren’t dangerous, but they’re inconvenient, costly, and add stress.
Patients with grafts often report more hospital trips than those with fistulas. One man in Auckland told his nurse, ‘I’ve had five procedures on my graft in two years. I wish I’d had the fistula when I had the chance.’
Still, for many, a graft is the only option. And with good care, it can serve well for years. The key? Watch for swelling, redness, pain, or warmth around the graft. Any of those could mean infection. And check for the thrill daily. If it’s gone, act fast.
Central Venous Catheter: The Temporary Fix That Often Stays Too Long
A central venous catheter is a soft tube inserted into a large vein in your neck, chest, or groin. It’s the only access that works immediately after placement. That’s why it’s often used for patients who need dialysis right away-like those who didn’t plan ahead or had sudden kidney failure.
But here’s the problem: catheters are the most dangerous option. They’re the main source of bloodstream infections in dialysis patients. The risk? 0.6 to 1.0 infections per 1,000 catheter days. That means if you’re on a catheter for 30 days, you have a 2% chance of getting a serious infection. And those infections? They often land you in the hospital.
Patients on catheters also face daily restrictions. You can’t shower normally. You must cover the site with waterproof dressing every time. No swimming. No hot tubs. No sleeping on the side where the catheter is. Many say it feels like living with a constant reminder that something’s wrong.
Worse, many people stay on catheters long after they should. Why? Because they’re afraid of surgery, or their veins aren’t suitable, or they don’t know better. But studies show that even patients with diabetes or older age can often still get a fistula-with proper planning. The real issue? Delayed referrals and lack of education.
Care Tips for Each Access Type
Good care can extend the life of any access. Here’s what you need to know:
- For Fistulas: Check for thrill every day. Wash your access arm with soap before every dialysis session. Don’t sleep on that arm. Don’t wear tight clothes or carry heavy bags on that side. Report any swelling, numbness, or pain right away.
- For Grafts: Same as fistulas-check for thrill. But be extra alert for signs of infection: redness, warmth, pus, or fever. Grafts need more monitoring. If you’ve had one for over a year, ask your doctor about ultrasound checks every 6 months.
- For Catheters: This is the most demanding. You must clean the caps every time you touch them. Use alcohol wipes. Never let the catheter ends touch anything dirty. Keep the dressing dry and clean. If it gets wet, change it immediately. Never let anyone else touch your catheter unless they’ve washed their hands and are trained. Report any fever, chills, or redness around the exit site immediately.
Patients who get trained early-before dialysis starts-have 25% fewer complications in the first year. That training includes how to check your access, how to spot trouble, and how to communicate with your care team. Don’t skip it.
What’s Changing in Dialysis Access?
Things are improving. The Fistula First Breakthrough Initiative, started in 2003, pushed hospitals and clinics to prioritize fistulas. In 2003, only 32% of U.S. dialysis patients had fistulas. By 2013, that number jumped to 65%. That’s progress.
New tech is helping too. In 2022, the FDA approved a wireless sensor called Vasc-Alert that monitors fistula blood flow daily. It sends alerts to your phone if flow drops, catching problems before they turn into clots. Early trials show a 20% drop in clotting events.
And research is looking ahead. Scientists are testing bioengineered blood vessels made from human tissue. One called Humacyte’s human acellular vessel is in late-stage trials. It could be a game-changer for patients with no healthy veins left.
But the biggest challenge remains: access inequality. Black patients are 30% less likely to get a fistula than White patients-even when they’re medically eligible. That’s not a medical issue. It’s a system issue. Delayed referrals, lack of education, and unequal access to vascular surgeons are still real.
What You Can Do Today
If you’re on dialysis or preparing for it:
- Ask for vein mapping before any surgery. Don’t assume you’re not a candidate.
- Request a fistula if you’re eligible-even if you think you need dialysis now. Many can wait 8 weeks with temporary care.
- Learn how to check your access daily. Know what ‘thrill’ feels like.
- Ask for training before your first treatment. Don’t wait until something goes wrong.
- If you’re on a catheter, ask your doctor: ‘Can I switch to a fistula or graft?’
Dialysis access isn’t just a medical procedure. It’s a lifestyle decision. The right access gives you freedom. The wrong one? It gives you fear.
What is the best type of dialysis access?
The best type is an arteriovenous (AV) fistula. It’s made from your own blood vessels, has the lowest risk of infection and clotting, and lasts the longest-often for decades. It’s the standard recommended by kidney health organizations worldwide.
Can I have a fistula if I have diabetes?
Yes, many people with diabetes can still get a fistula. Diabetes can damage blood vessels, but vein mapping (an ultrasound scan) helps doctors determine if your vessels are strong enough. Even if your veins are smaller, a skilled vascular surgeon can often find a suitable location. Preoperative exercise programs have also been shown to improve fistula success in diabetic patients.
How long does it take for a fistula to be ready for use?
It usually takes 6 to 8 weeks for a fistula to mature. During this time, the vein grows larger and stronger from the increased blood flow. Some fistulas take longer, especially in older patients or those with diabetes. Your care team will monitor it with ultrasound to know when it’s ready.
Why do catheters have higher infection rates?
Catheters are tubes that sit directly in large veins and stick out of the skin. This creates a direct path for bacteria to enter your bloodstream. Even with careful cleaning, daily handling, moisture, and movement increase infection risk. Fistulas and grafts are under the skin and don’t have an open exit point, making them far safer.
What should I do if I lose the thrill in my fistula?
If you can’t feel the vibration (thrill) in your fistula, call your dialysis center immediately. This could mean a clot has formed or the vessel has narrowed. Quick action-often within 24 hours-can prevent permanent damage. Most clots can be cleared with a simple procedure if caught early.
Can I shower normally with a graft or fistula?
Yes, you can shower normally with a fistula or graft. You don’t need special dressings unless you’ve just had surgery or have an open wound. After the initial healing period (about 1-2 weeks), your access site is protected under the skin. Just avoid scrubbing it directly. Catheters, however, require waterproof coverings every time you shower.
How often should my dialysis access be checked?
Fistulas and grafts should be checked at every dialysis session by your nurses. They’ll feel for the thrill and listen for a bruit (a whooshing sound). For long-term users, an ultrasound check every 6 to 12 months is recommended to catch narrowing before it causes a clot. Catheters need daily inspection for signs of infection or leakage.
Is it safe to exercise with a dialysis access?
Yes, exercise is encouraged-especially before fistula surgery. Light to moderate activity like walking, cycling, or arm exercises can improve blood flow and increase the chance your fistula will mature successfully. After surgery, avoid heavy lifting or pressure on the access arm for 2-4 weeks. Once healed, normal activity is safe.
What’s Next?
If you’re on dialysis, don’t accept catheter use as your only option. Ask questions. Push for vein mapping. Request a fistula if you’re eligible. If you’ve been on a catheter for months, talk to your nephrologist about transitioning. The goal isn’t just to survive dialysis-it’s to live well while you’re on it.
And if you’re helping someone else-family, a friend, a caregiver-learn how to check for the thrill. Know the signs of trouble. Be their advocate. Because in dialysis, the best care doesn’t always come from a machine. Sometimes, it comes from a simple, daily check of a vein.
















14 Comments