
Warfarin saves lives. It prevents deadly blood clots in people with atrial fibrillation, artificial heart valves, or a history of deep vein thrombosis. But for every person who finds stability on warfarin, there’s another who ends up in the ER because of something they ate, took, or didn’t realize was dangerous. This isn’t scare tactics-it’s reality. Warfarin doesn’t play nice. It has over 297 known interactions, and even small changes can send your INR sky-high or crash it too low. If you’re on warfarin, you’re not just taking a pill. You’re managing a delicate system where a bowl of spinach, a new antibiotic, or a daily vitamin can flip your clotting risk overnight.
How Warfarin Works (And Why It’s So Sensitive)
Warfarin doesn’t thin your blood like water. It blocks vitamin K, a nutrient your liver needs to make clotting factors. Without enough active vitamin K, your blood takes longer to clot-and that’s the whole point. But here’s the catch: your body doesn’t store vitamin K like it does vitamin C. You need a steady, predictable amount every day. If you eat a huge plate of kale on Monday and none all week, your INR will bounce around like a ping-pong ball. The goal? Keep your INR between 2.0 and 3.0. Go above 3.5? You risk bleeding. Below 2.0? You risk clots. That narrow window is why warfarin demands precision.
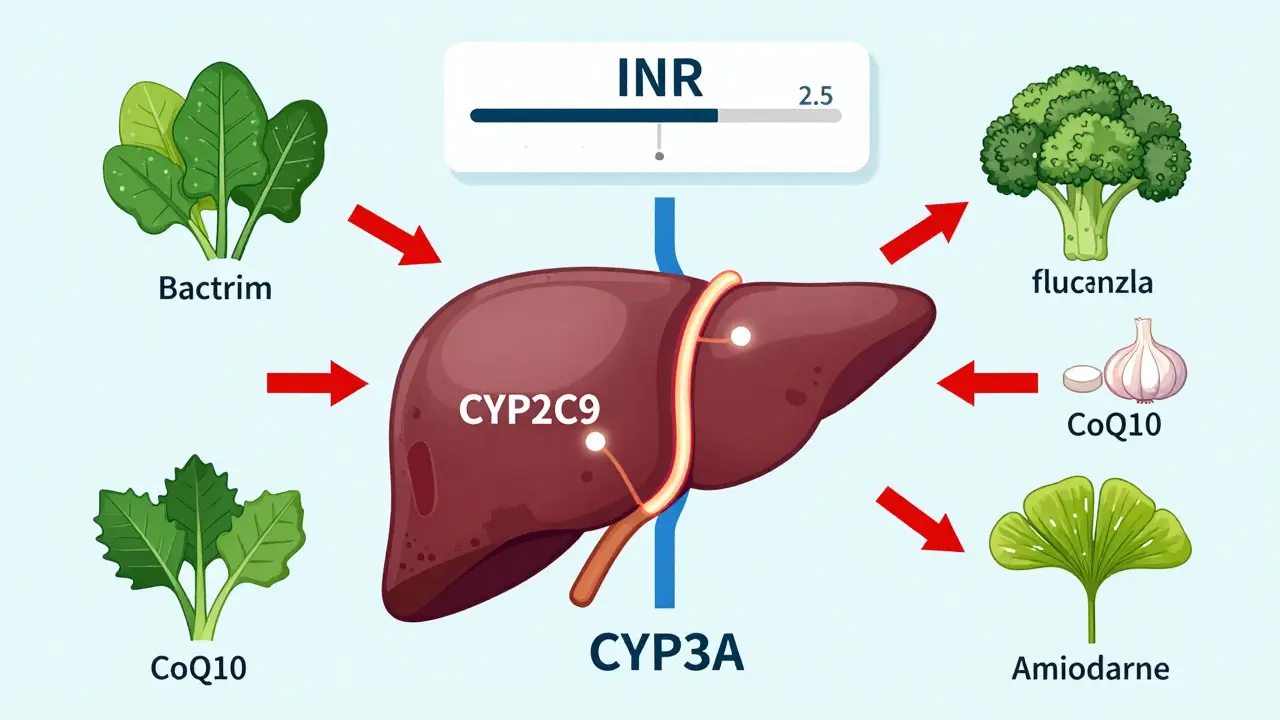
Warfarin’s half-life is 20 to 60 hours. That means it sticks around for days. A single dose can affect your clotting for nearly a week. It’s broken down by liver enzymes-mainly CYP2C9 and CYP3A4. If something blocks or speeds up these enzymes, your warfarin levels go haywire. That’s why antibiotics, antifungals, and even herbal teas can trigger dangerous changes. Unlike newer blood thinners, warfarin has no built-in safety net. You can’t just take it and forget it. You have to monitor, adjust, and be vigilant.
Foods That Change Your INR
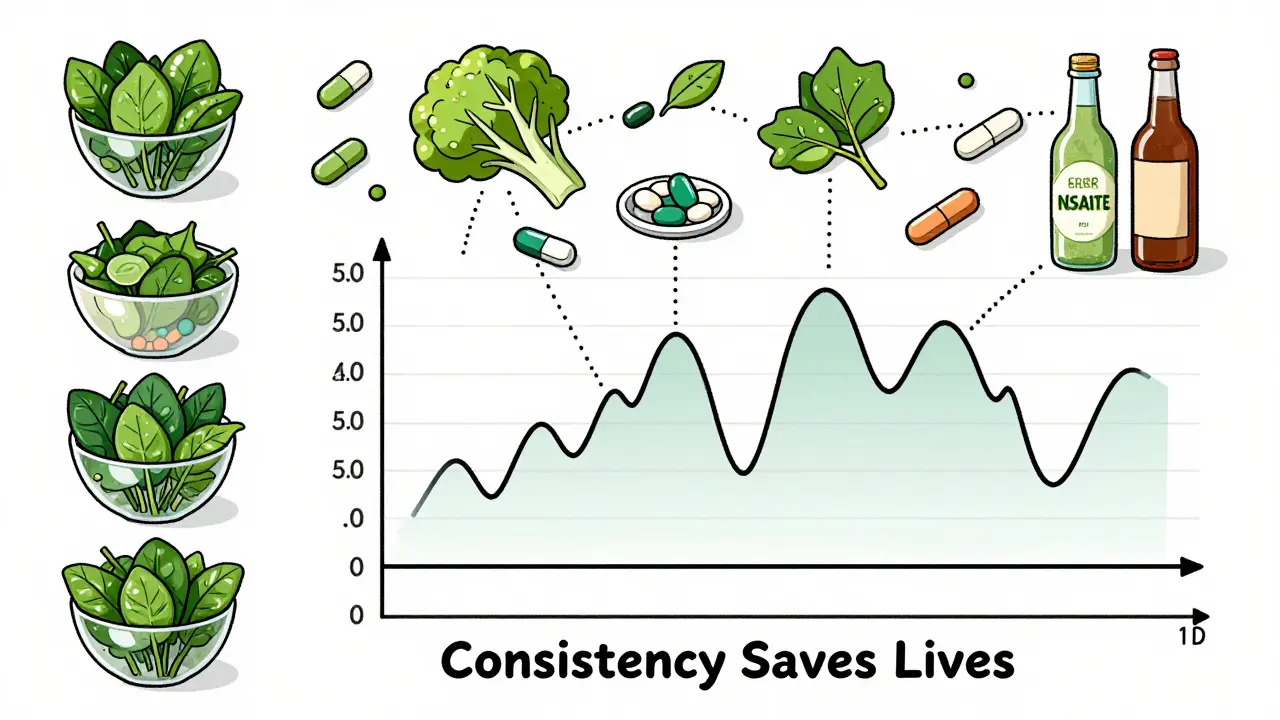
Vitamin K is the biggest dietary player. It’s not evil. It’s essential. But if you’re on warfarin, consistency is everything. You don’t need to avoid vitamin K-rich foods-you need to eat the same amount every day.
- Leafy greens: Spinach, kale, collards, Swiss chard, and broccoli are packed with vitamin K. One cup of cooked spinach has 1,062 mcg. One cup of cooked broccoli? 220 mcg. If you normally eat one serving a week and suddenly eat three, your INR can drop 0.5-1.5 points in just a few days.
- Other sources: Green tea, soybean oil, and canola oil also contain vitamin K. Soy products like tofu and edamame can interfere too-especially if you suddenly increase your intake.
- What to do: Pick one or two consistent sources and stick with them. A 2022 patient survey found that those who ate exactly one cup of cooked spinach daily at the same time (usually dinner) had the most stable INR levels. Don’t go on a kale cleanse. Don’t skip your greens for a week. Just keep it steady.
Alcohol is another silent disruptor. One or two drinks a day? Usually fine. Three or more? That triples your bleeding risk. Alcohol affects liver enzymes and can also cause dehydration, which thickens your blood and makes INR harder to predict. If you drink regularly, don’t suddenly quit. If you don’t drink, don’t start.
Supplements That Can Be Dangerous
"Natural" doesn’t mean safe. Many supplements interact with warfarin-and most people don’t realize it.
- Garlic, ginger, ginkgo biloba: These are common in supplements for circulation or brain health. But they have antiplatelet effects. They don’t change your INR directly, but they increase bleeding risk on their own. Combine them with warfarin? You’re doubling down on risk.
- Coenzyme Q10 (CoQ10): Often taken for heart health or statin side effects. It acts like vitamin K in your body. A single 100 mg dose can lower your INR enough to require a warfarin dose increase.
- St. John’s Wort: This herb is used for mild depression. It speeds up the CYP3A4 enzyme, causing warfarin to break down faster. INR drops. Clots form. There are documented cases of strokes in people who started St. John’s Wort while on warfarin.
- Vitamin E: High doses (over 400 IU/day) can increase bleeding risk. Most multivitamins are fine. But if you’re taking extra vitamin E for "heart health," stop. Talk to your doctor.
- Green tea extract: Not the same as drinking tea. Supplements concentrate the compounds. One case report showed a patient’s INR dropped from 3.2 to 1.8 after starting green tea extract. Her doctor had to increase her warfarin dose by 40%.
Bottom line: Never start a new supplement without checking with your anticoagulation clinic. Even something as simple as a fish oil pill can matter. Keep a log. Tell your pharmacist. Bring your supplement bottle to every appointment.
Prescription Drugs That Change Everything
Drug interactions are the most dangerous part of warfarin therapy. Over 70% of serious incidents happen because of medication changes.
- Antibiotics: Especially trimethoprim-sulfamethoxazole (Bactrim), ciprofloxacin, and metronidazole. These block the enzyme that breaks down warfarin. INR spikes. Bleeding follows. One patient on Reddit reported an INR of 5.1 after taking Bactrim for a UTI-three ER visits later.
- Antifungals: Fluconazole (Diflucan) increases warfarin levels by 50-100%. Doctors often cut the warfarin dose by 25-50% before even starting the antifungal.
- Amiodarone: Used for irregular heart rhythms. It’s one of the most dangerous interactions. It can double warfarin levels. Many patients need a 30-50% dose reduction when starting amiodarone.
- NSAIDs: Ibuprofen, naproxen, celecoxib. These don’t change INR, but they irritate the stomach lining. Combine that with warfarin’s blood-thinning effect, and you’re asking for a GI bleed. Acetaminophen (Tylenol) is safer for pain.
- SSRIs: Some antidepressants like fluoxetine and sertraline can increase bleeding risk. They don’t always change INR, but they affect platelets. If you’re on warfarin and need an antidepressant, ask about citalopram or escitalopram-they’re lower risk.
Always check new prescriptions with your pharmacist. Don’t assume your doctor knows every interaction. Many don’t. A 2021 study found that nearly 40% of warfarin patients received a new drug that interacted with their anticoagulant, and their doctor didn’t adjust the dose.
What to Do If You’re on Warfarin
Stability is everything. Here’s how to stay safe:
- Test your INR regularly. Even if you feel fine. Most people need testing every 4 weeks when stable. Don’t skip. Your INR can change without symptoms.
- Keep a food and medication log. Write down everything you eat, drink, and take-including over-the-counter pills and herbal teas. Bring it to every appointment.
- Never start or stop anything without checking. That includes vitamins, supplements, cold medicines, and herbal remedies. Even OTC pain relievers can be risky.
- Know the signs of bleeding. Unusual bruising, nosebleeds that won’t stop, pink or red urine, dark stools, headaches, or dizziness could mean your INR is too high. Call your doctor immediately.
- Wear a medical alert bracelet. In an emergency, paramedics need to know you’re on warfarin. It could save your life.
Warfarin vs. Newer Blood Thinners
Many people wonder: Why not just switch to Eliquis or Xarelto? Those drugs have fewer interactions. No INR tests. Just take them daily.
But here’s the reality: Warfarin still has a place. For people with mechanical heart valves, DOACs (direct oral anticoagulants) aren’t safe-they don’t work well enough. For people with severe kidney failure, DOACs can build up to toxic levels. And for those on Medicare, warfarin costs $80 a year. DOACs? Around $6,500.
So if you’re on warfarin, you’re not stuck with an outdated drug. You’re managing a powerful tool-one that demands respect. It’s not about fear. It’s about control. You can live well on warfarin. But you have to be smart about it.
What’s Changing Now?
There’s new hope. In 2023, the FDA approved a genetic test called Warfarin GenAssist. It looks at your CYP2C9 and VKORC1 genes to predict how you’ll respond to warfarin. This can cut the time to reach stable INR by over two weeks. Early data shows it reduces dangerous INR swings by 40%.
Also, AI dosing tools are now being tested. One model from 2023 predicted the right warfarin dose with 82% accuracy-better than most doctors using traditional methods. These won’t replace your clinic, but they’ll help them get you stable faster.
Still, the basics haven’t changed. Food. Supplements. Drugs. Consistency. Monitoring. That’s the core of safe warfarin use.
Can I eat spinach if I’m on warfarin?
Yes-but only if you eat the same amount every day. One cup of cooked spinach has over 1,000 mcg of vitamin K. If you normally eat it twice a week and suddenly eat it every day, your INR will drop. If you skip it for a week, your INR will rise. Consistency matters more than avoidance.
Does green tea interact with warfarin?
Drinking 1-2 cups of green tea daily is usually fine. But green tea extract pills? Those can lower your INR significantly. One case study showed a patient’s INR dropped from 3.2 to 1.8 after starting a supplement. Stick to tea, not pills.
Can I take ibuprofen with warfarin?
No. Ibuprofen and other NSAIDs increase your risk of stomach bleeding when combined with warfarin. Use acetaminophen (Tylenol) instead for pain or fever. Always check with your doctor before taking any pain reliever.
How long does it take for a new drug to affect my INR?
It varies. Antibiotics like Bactrim can raise your INR within 2-3 days. Fluconazole can spike levels in under 48 hours. Some interactions take weeks. Always notify your anticoagulation clinic when you start or stop any medication-even if it’s just for a few days.
Why do I need to test my INR if I feel fine?
Warfarin doesn’t cause symptoms when it’s too high or too low. You can have an INR of 6.0 and feel perfectly normal-but you’re at high risk of internal bleeding. Or your INR could be 1.5 and you’re not protected from clots. Testing catches changes before they become emergencies.
Warfarin isn’t going away. It’s still the go-to for millions of people who need a reversible, affordable, and reliable anticoagulant. But it’s not a passive medication. It’s a partnership. You have to show up. Track what you eat. Report every new pill. Stick to your testing schedule. The more consistent you are, the safer you are. And that’s the only way to live well on warfarin.











9 Comments