

Have you ever wondered why a bottle of generic atorvastatin costs pennies at one pharmacy but dollars more at another? Or why that specific blood pressure medication is suddenly out of stock everywhere? The answer isn't just about the pill itself. It’s about a complex, often opaque web of manufacturers, wholesalers, and middlemen that controls how generic drugs move from a factory floor to your hands.
When you pick up a prescription, you’re seeing the final step in a journey that spans continents. Understanding this generic drug supply chain reveals why prices fluctuate, where shortages come from, and who actually profits when you pay for your medicine. It’s not as simple as 'manufacturer makes it, pharmacy sells it.' There are powerful players in between shaping every dollar and every decision.
Where Generic Drugs Actually Come From
The story starts long before a tablet is pressed. It begins with Active Pharmaceutical Ingredients (APIs). These are the pure chemical substances that make the drug work. Here is the shocker: only about 12 percent of these critical ingredients are manufactured in the United States. According to a 2021 study published in PMC, roughly 88 percent of API production happens overseas, primarily in China and India.
This global dependency creates a fragile link. If a factory in India faces a power outage or a port in Shanghai closes due to weather, the ripple effect hits U.S. pharmacies weeks later. During the COVID-19 pandemic, this vulnerability became painfully clear when API shortages affected over 170 generic medications. Manufacturers here rely on those distant suppliers because labor and regulatory costs are significantly lower abroad, but it means quality control becomes a logistical nightmare for regulators like the FDA.
Once the APIs arrive, U.S.-based or local contract manufacturers turn them into finished pills. But they can’t just start selling. They must secure approval through an Abbreviated New Drug Application (ANDA). This process proves their version is therapeutically equivalent to the original brand-name drug. Unlike brand companies that spend billions on clinical trials, generics skip that step by relying on existing data, which is why they are cheaper to produce-but the regulatory hurdle remains high to ensure safety.
The Middlemen: Wholesalers and Distributors
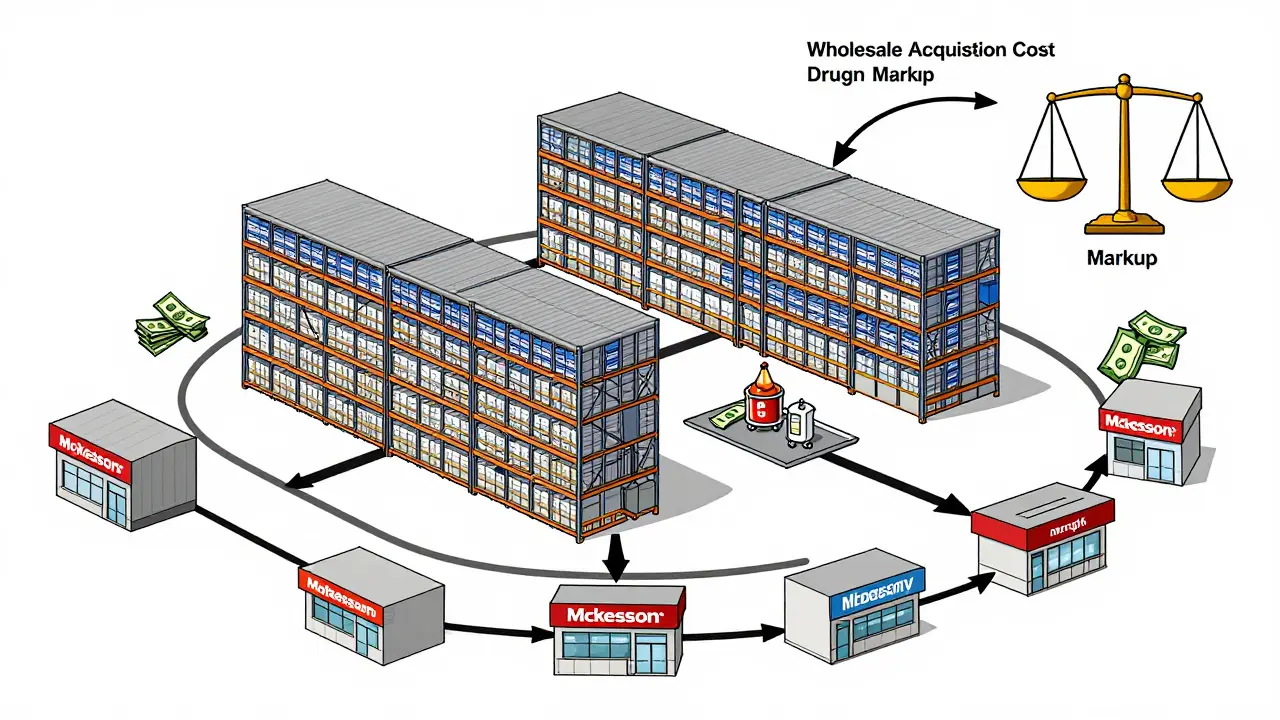
After the pills are made, they don’t go straight to the pharmacy down the street. They go to wholesale distributors. Think of companies like McKesson, AmerisourceBergen, and Cardinal Health. These giants act as the central hub of the supply chain. Manufacturers sell to them in massive bulk, and these wholesalers then break down those orders to feed thousands of independent pharmacies, hospital systems, and retail chains.
Why do we need them? Efficiency. A small pharmacy cannot store enough inventory to cover every possible prescription request. Wholesalers hold the stock so pharmacies can order what they need, when they need it. However, this relationship involves heavy negotiation. Wholesalers offer "prompt payment discounts"-essentially giving manufacturers a kickback if they pay invoices quickly. In return, wholesalers charge pharmacies a markup on the Wholesale Acquisition Cost (WAC). This markup varies wildly based on the pharmacy’s size and bargaining power. Large chains get better rates; independents often pay more, squeezing their already thin margins.
The PBM Powerhouse: Who Really Controls the Price?
If wholesalers handle the logistics, Pharmacy Benefit Managers (PBMs) handle the money-and the rules. PBMs like CVS Caremark, OptumRx, and Express Scripts process the vast majority of prescriptions in the U.S. They sit between insurance companies and pharmacies, deciding which drugs are covered, how much patients pay, and crucially, how much pharmacies get reimbursed.
For brand-name drugs, PBMs negotiate huge rebates from manufacturers in exchange for placing those drugs on preferred lists. But generics are different. As noted in the Association for Accessible Medicines' 2024 brief, generic manufacturers rarely engage in rebate negotiations. Instead, PBMs use a method called Maximum Allowable Cost (MAC). MAC sets a hard ceiling on what a pharmacy will be paid for a specific generic drug, regardless of what the pharmacy actually paid to buy it.
This system creates a dangerous gap. If the MAC price is set lower than the pharmacy’s actual acquisition cost, the pharmacy loses money every time they fill that prescription. A 2023 survey by the American Pharmacists Association found that 68 percent of independent pharmacy owners cited MAC pricing below acquisition cost as a major financial pressure. Some pharmacies even refuse to stock certain generics because dispensing them guarantees a loss.
Generic vs. Brand: Two Different Worlds
To understand the stress on the generic supply chain, you have to compare it to the brand-name world. The structures look similar but operate under completely different economic rules.
| Feature | Generic Drugs | Brand-Name Drugs |
|---|---|---|
| Manufacturer Revenue Share | ~36% of total expenditure | ~76% of total expenditure |
| Reimbursement Method | Maximum Allowable Cost (MAC) | Percentage of List Price + Rebates |
| Pricing Control | Low (intense competition) | High (patent protection) |
| API Sourcing | 88% Overseas (China/India) | Mixed, often higher domestic content |
| Market Concentration | Top 10 makers control 65% | Fragmented across many big pharma firms |
Notice the revenue share disparity. While brand manufacturers keep most of the money spent on their products, generic manufacturers capture only about a third. Why? Because half of the revenue goes directly to production costs, and the rest is absorbed by intermediaries. This "race to the bottom" pricing dynamic means generic companies operate on razor-thin margins. When raw material costs rise or shipping delays occur, there is no buffer. This fragility is exactly why shortages happen so frequently in the generic market.

Why Shortages Keep Happening
You’ve likely seen empty shelves for common antibiotics or painkillers. This isn’t accidental. It’s a symptom of a supply chain stretched too thin. With margins so low, manufacturers have little incentive to maintain extra inventory. If demand spikes unexpectedly, they can’t ramp up production quickly because API supplies are fixed and overseas.
Furthermore, market consolidation has made things worse. The top ten generic manufacturers now control 65 percent of the U.S. market. If one of these few companies halts production due to a quality issue or inspection failure, there may be no other supplier ready to step in immediately. The FDA has increased inspections of foreign facilities-from 248 in 2010 to 641 in 2022-but monitoring hundreds of overseas plants remains a challenge. When a facility fails inspection, shipments stop, and pharmacies scramble.
The Future: Technology and Transparency
The industry knows something has to change. Recent analyses point toward technology as the savior of the generic supply chain. Concepts like blockchain are being tested to create immutable records of drug movement, ensuring authenticity and tracking bottlenecks in real-time. AI-driven demand forecasting helps wholesalers predict surges in demand before they lead to shortages.
Policy shifts are also coming. The Inflation Reduction Act of 2022 introduced new Medicare pricing provisions that could reshape how generics are reimbursed, potentially easing some pressure on pharmacies. Meanwhile, the FDA’s Drug Competition Action Plan aims to streamline approvals and improve communication with manufacturers during crises. Diversified sourcing strategies are becoming standard best practices, with companies actively seeking to reduce reliance on single geographic regions for APIs.
Until these changes fully take root, the generic drug supply chain remains a delicate balance. It delivers affordable medicine to millions, but its complexity hides significant risks. For patients, understanding this landscape explains why availability and price aren’t always predictable-and why supporting local pharmacies and staying informed about drug alternatives matters more than ever.
Why are generic drugs so cheap compared to brand names?
Generic drugs are cheaper because manufacturers don’t have to repeat expensive clinical trials. They only need to prove their product is bioequivalent to the brand name via an Abbreviated New Drug Application (ANDA). Additionally, intense competition among multiple generic manufacturers drives prices down, whereas brand-name drugs benefit from patent exclusivity that allows higher pricing.
What causes generic drug shortages?
Shortages often stem from the reliance on overseas Active Pharmaceutical Ingredient (API) suppliers, primarily in China and India. Disruptions in manufacturing, shipping, or regulatory inspections can halt production. Since generic margins are thin, manufacturers keep minimal inventory, making the supply chain vulnerable to sudden demand spikes or production failures.
How do PBMs affect pharmacy reimbursement for generics?
Pharmacy Benefit Managers (PBMs) often use Maximum Allowable Cost (MAC) pricing for generics. This sets a maximum reimbursement rate for pharmacies. If the MAC price is lower than what the pharmacy paid to acquire the drug, the pharmacy loses money on the sale. This differs from brand drugs, which typically involve rebate negotiations rather than strict caps.
Where are most generic drug ingredients made?
Approximately 88 percent of Active Pharmaceutical Ingredients (APIs) used in U.S. generic drugs are manufactured outside the United States, mainly in China and India. Only about 12 percent of API production occurs domestically, creating significant supply chain dependencies and potential vulnerabilities.
Who makes the most money in the generic drug supply chain?
Surprisingly, generic manufacturers capture only about 36 percent of the total expenditure on generic drugs. The remaining majority is taken by intermediaries such as wholesalers, Pharmacy Benefit Managers (PBMs), and payers. In contrast, brand-name manufacturers retain about 76 percent of expenditures, highlighting the structural differences in profit distribution.












9 Comments