
DI-AKI Risk Assessment Tool
How to Use This Tool
Answer the questions below to get a personalized assessment of your risk for drug-induced kidney injury. This tool is based on the latest medical guidelines including KDIGO 2024 recommendations. Results are for informational purposes only and should not replace professional medical advice.
Your Risk Assessment
Every year, thousands of people end up in the hospital with sudden kidney failure-not from an infection, not from trauma, but from a pill they took for a headache, a backache, or even an infection. This isn’t rare. In fact, drug-induced kidney injury (DI-AKI) is responsible for up to 60% of all acute kidney injuries in intensive care units. And here’s the hard truth: most of these cases are preventable.
What Exactly Is Drug-Induced Kidney Failure?
Drug-induced kidney failure, or drug-induced acute kidney injury (DI-AKI), isn’t one single problem. It’s a group of conditions caused by medications that damage the kidneys in different ways. The kidneys filter waste and balance fluids, but certain drugs interfere with that process. This can happen fast-sometimes within hours-or over days. The result? A sudden drop in kidney function, measured by rising creatinine levels or low urine output.
The most common triggers? Antibiotics like vancomycin and piperacillin-tazobactam, painkillers like ibuprofen and naproxen, and even common heartburn meds like omeprazole. Contrast dyes used in CT scans and some HIV drugs also top the list. According to the KDIGO 2024 guidelines, DI-AKI is defined by any of these: a creatinine increase of 0.3 mg/dL or more within 48 hours, a 50% rise from baseline, or urine output below 0.5 mL per kg per hour for six hours straight.
What makes this especially dangerous is that many people don’t realize their kidneys are at risk. They take a drug because it’s over-the-counter, or their doctor prescribed it without checking kidney function first. And by the time symptoms show up-fatigue, swelling, confusion, or no urine at all-it’s often too late to fully recover.
How Do Drugs Actually Damage the Kidneys?
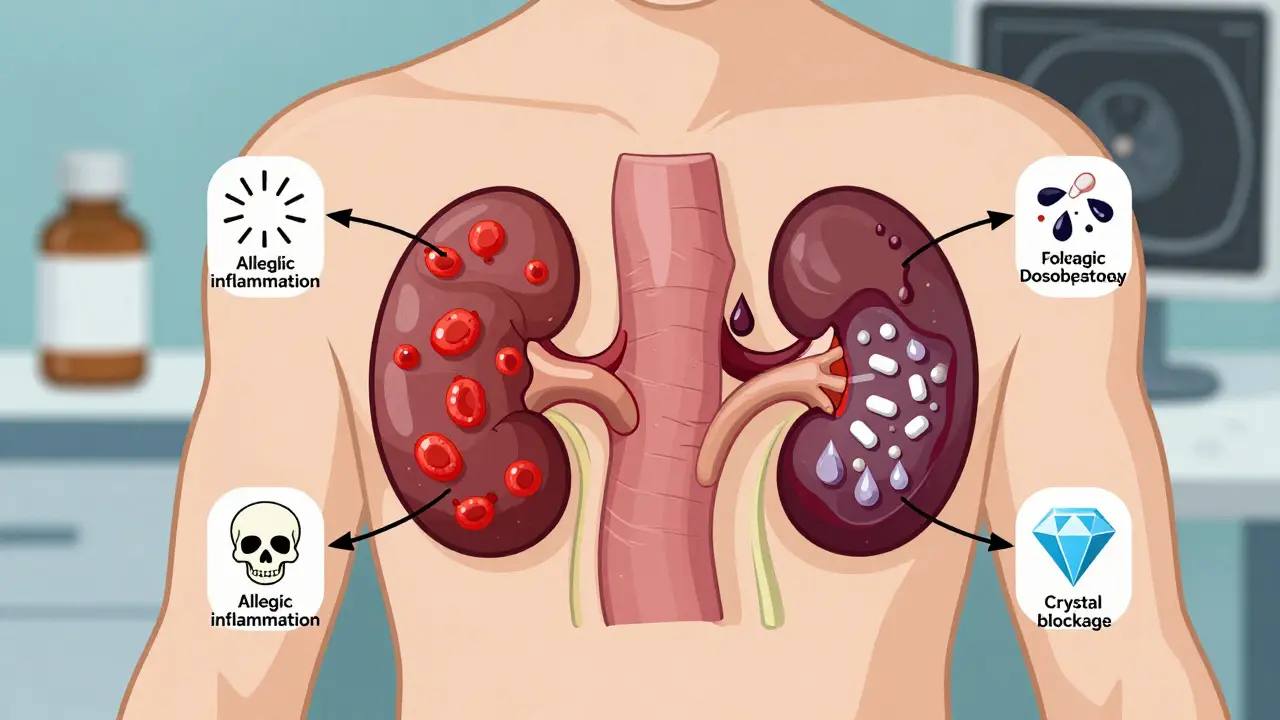
Not all kidney damage from drugs works the same way. There are three main mechanisms:
- Acute interstitial nephritis: This is an allergic-type reaction where the immune system attacks the space between kidney tubules. It’s most often caused by proton pump inhibitors (like omeprazole), penicillin antibiotics, and NSAIDs. Symptoms usually appear 7 to 14 days after starting the drug: fever, rash, joint pain, and sometimes blood in the urine.
- Acute tubular necrosis: This is direct poisoning of the kidney’s filtering tubes. Drugs like aminoglycosides (gentamicin), vancomycin, and contrast dyes cause this. It’s common in ICU patients who get multiple strong drugs at once.
- Crystal-induced nephropathy: Some drugs form crystals in the urine that clog the tubules. Think acyclovir (for herpes), sulfonamides (like Bactrim), and certain HIV meds. These crystals can cause sudden kidney failure within hours. The good news? It’s often reversible if caught early and you drink enough water to flush them out.
For example, sulfadiazine-used for urinary tract infections-can cause crystal buildup if urine is too acidic. Keeping urine pH above 7.1 and drinking at least 3 liters of water a day prevents this. Simple? Yes. Often ignored? Also yes.
Who’s Most at Risk?
Not everyone who takes a nephrotoxic drug will develop kidney injury. But some people are sitting ducks:
- People over 65
- Those with existing kidney disease (eGFR below 60 mL/min/1.73m²)
- Diabetics or people with heart failure
- Anyone on multiple medications (5 or more)
- Patients who are dehydrated or on diuretics
One study found that polypharmacy-taking five or more drugs at once-doubles the risk of DI-AKI. And it’s not just about the drugs themselves. It’s how they interact. For example, combining NSAIDs with ACE inhibitors (common for blood pressure) in someone with reduced kidney function can cause sudden failure. This combo is sometimes called the “triple whammy” when a diuretic is added.
Here’s a real case: A 72-year-old man with stage 3 chronic kidney disease took ibuprofen for 10 days after dental surgery. His creatinine jumped from 1.8 to 4.2 in three days. He ended up hospitalized for a week. His doctor didn’t connect the dots until it was too late. This isn’t an outlier. Patient forums show 54% of DI-AKI cases involve delayed recognition.

Recognizing the Signs Early
DI-AKI often flies under the radar. You won’t feel your kidneys failing. But there are clues:
- Sudden drop in urine output (less than half your usual)
- Swelling in legs, ankles, or face
- Unexplained fatigue, nausea, or confusion
- Fever or rash that appeared after starting a new drug
- High blood pressure that’s suddenly harder to control
Doctors rely on blood tests. A creatinine increase of 0.3 mg/dL or more within 48 hours is a red flag. But many hospitals don’t check creatinine before prescribing high-risk drugs. In fact, 31% of DI-AKI cases occur because baseline kidney function was never measured.
And here’s the kicker: some patients don’t even know they have kidney disease. A 2023 study found that 40% of people with eGFR below 60 had never been told. If you’re over 50, have high blood pressure, or take regular painkillers, ask for a simple blood test. It takes five minutes.
Prevention: The 3 Rs Framework
Preventing drug-induced kidney injury isn’t rocket science. It’s about systems, not just individual choices. The NHS Kidney Care team calls it the “three Rs”:
- Reduce risk: Avoid nephrotoxic drugs when possible. For example, use acetaminophen instead of ibuprofen for pain if you have kidney issues. NSAIDs increase AKI risk by 47% in people with eGFR below 60. That’s not a small number-it’s a game-changer.
- Recognize early: Always check kidney function before starting high-risk medications. This includes antibiotics, contrast dyes, and even some blood pressure pills. If you’re getting a CT scan with contrast, ask if your creatinine was checked in the last 30 days. If not, insist on it.
- Right response: If kidney function drops, stop the offending drug immediately. Don’t wait for symptoms to worsen. In one study, patients who had their nephrotoxic drug stopped within 24 hours of a creatinine spike had 70% less chance of needing dialysis.
Electronic health records with built-in renal dosing alerts cut inappropriate prescribing by 63%. That’s huge. If your doctor’s office doesn’t have this system, ask why. It’s not a luxury-it’s a safety net.
What About Common Drugs Like NSAIDs and Contrast Dye?
NSAIDs (ibuprofen, naproxen, celecoxib) are the most common offenders. They’re in almost every medicine cabinet. But here’s what most people don’t know: in someone with existing kidney disease, even a few days of NSAIDs can trigger acute failure. The FDA has required black box warnings on these drugs since 2005. Yet they’re still sold over the counter like candy.
Contrast dye used in CT scans causes about 10% of hospital-acquired AKI. But we know how to prevent it. Hydration with normal saline before and after the scan reduces risk by 28%. High-dose statins (like atorvastatin 80mg) taken 24 hours before the scan lower risk by 34%. Sodium bicarbonate? Doesn’t help. N-acetylcysteine? No convincing proof. Stick to what works: fluids and statins.
And don’t assume your doctor knows. A 2019 UK audit found that 38% of AKI cases happened because nephrotoxic drugs were continued despite clear kidney damage. That’s not negligence-it’s systemic failure.
What You Can Do Right Now
You don’t need to be a doctor to protect your kidneys. Here’s your action plan:
- Ask your doctor for an eGFR test if you’re over 50 or have diabetes, high blood pressure, or heart disease.
- Keep a list of all your medications-including supplements and OTC painkillers-and review it with your doctor every six months.
- Never take NSAIDs for more than 3 days in a row if you have kidney disease or are over 65.
- If you’re scheduled for a CT scan, ask: “Was my kidney function checked? Do I need hydration before and after?”
- If you’re on multiple drugs, ask: “Could any of these hurt my kidneys?”
One patient, MaryK_65, shared on a kidney forum: “My cardiologist switched me from naproxen to acetaminophen after my eGFR dropped to 52. My kidney function stabilized in two weeks.” That’s the power of awareness.
The Bigger Picture: Costs and Progress
DI-AKI isn’t just a health issue-it’s a financial one. In the U.S., each episode costs an average of $18,450. Annually, drug-related kidney injuries add up to $1.2 billion in avoidable costs. And that’s just in hospitals. Add in ER visits, dialysis, and long-term care, and the number explodes.
But there’s hope. In 2024, the FDA approved the first AI system-Dosis Health-that predicts which patients are at risk of DI-AKI before they even take a drug. In a trial of over 15,000 patients, it cut kidney injury cases by 41%. That’s not science fiction. It’s here.
The American Society of Nephrology aims to cut preventable DI-AKI by 50% by 2030. They’re not waiting. Hospitals are rolling out protocols. Pharmacies are updating alerts. Patients are being educated.
The message is clear: kidney damage from drugs isn’t inevitable. It’s a system failure. And systems can be fixed.

















12 Comments