
When you're prescribed a blood thinner, you're not just getting a pill-you're signing up for a daily balancing act. One wrong move, and you could bleed internally. Skip a dose, and a clot might form. Two drugs dominate this high-stakes game: warfarin and direct oral anticoagulants (DOACs) a class of newer blood thinners including apixaban, rivaroxaban, dabigatran, and edoxaban. Both prevent strokes and clots, but their safety profiles, daily burdens, and risks couldn't be more different.
How Warfarin Works-and Why It’s Still Around
Warfarin has been the go-to blood thinner since the 1950s. It works by blocking vitamin K, which your body needs to make clotting factors. Simple in theory, messy in practice. It takes 3 to 5 days to start working, and even then, it’s unpredictable. Your INR (International Normalized Ratio) must stay between 2.0 and 3.0. Too low? You risk a stroke. Too high? You could bleed out.
That’s why people on warfarin get frequent blood tests. The first month? You might need 6 to 12 tests. After that? At least 2 to 4 per month. And if your INR is off? You get a call from your doctor, maybe a dose change, or even a hospital visit. It’s exhausting. Plus, warfarin interacts with over 300 medications and dozens of foods. Spinach, kale, broccoli-even a big salad can throw your INR off. Alcohol? Antibiotics? Even some herbal supplements? They all play a role.
Despite all this, warfarin still has a place. If you have a mechanical heart valve, DOACs won’t work. Period. The same goes for severe kidney failure (eGFR below 15). In those cases, warfarin is the only option that’s been proven safe and effective.
DOACs: The New Standard-But Not Perfect
DOACs-like apixaban (Eliquis®), rivaroxaban (Xarelto®), dabigatran (Pradaxa®), and edoxaban (Savaysa®)-changed the game. They don’t need INR checks. You take the same dose every day. No food restrictions. Fewer drug interactions. And according to data from the American Heart Association (2024), they’re safer overall.
For atrial fibrillation patients, DOACs cut stroke risk by 30% compared to warfarin. They also slash the chance of dangerous brain bleeds by 50%. That’s huge. In fact, as of 2023, DOACs made up 78% of all anticoagulant prescriptions in the U.S. Apixaban alone accounted for nearly 40% of the market.
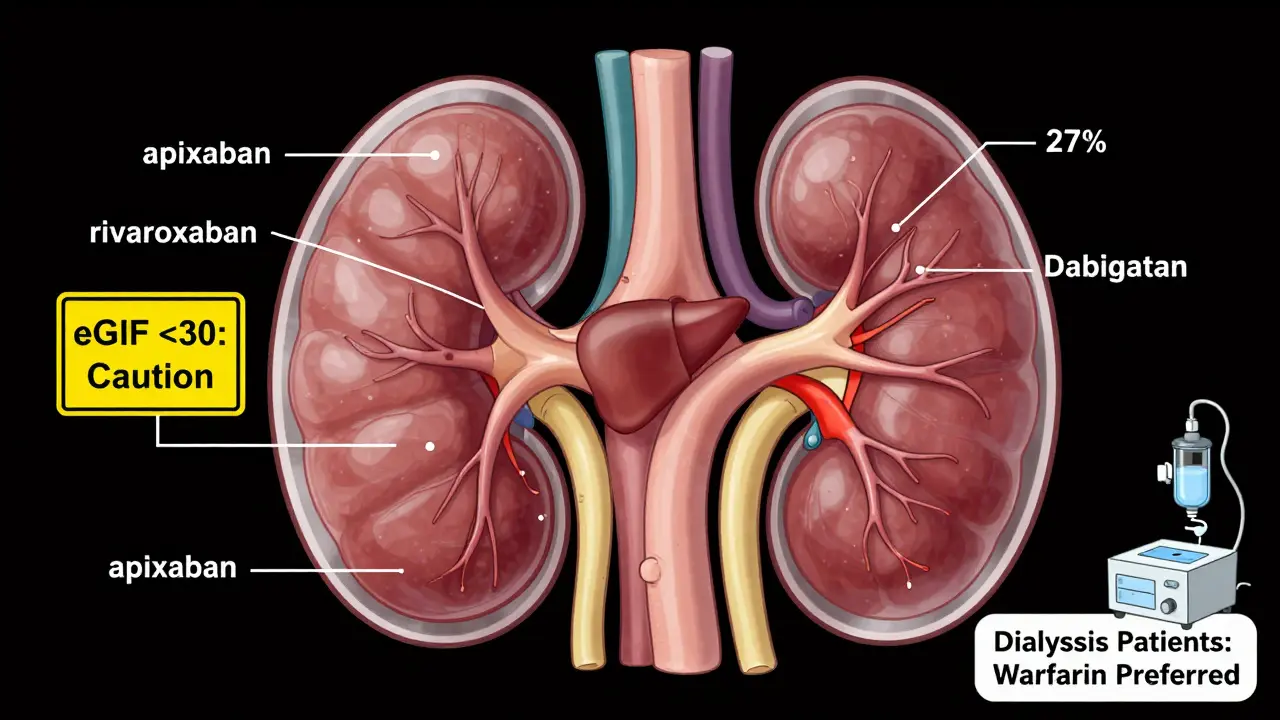
But DOACs aren’t magic. They’re cleared through your kidneys. If your kidney function drops below 30 mL/min, some DOACs become risky. Dabigatran? 80% of it leaves through your kidneys. Apixaban? Only 27%. That’s why doctors check your eGFR before prescribing. And if you have advanced kidney disease-especially if you’re on dialysis-DOACs aren’t always the answer.
Also, there’s no universal antidote. If you overdose or need emergency surgery, reversal agents exist-but only for some. Andexanet alfa reverses apixaban and rivaroxaban. Idarucizumab reverses dabigatran. Edoxaban? No approved reversal agent yet. Warfarin? Vitamin K and fresh plasma can fix it fast.
Which One Is Safer? The Data Says
Let’s cut through the noise. Here’s what the latest studies show:
- Major bleeding: DOACs reduce major bleeding by 28% compared to warfarin. Apixaban has the lowest risk among DOACs.
- Intracranial hemorrhage: DOACs cut brain bleeds by half. This is the deadliest kind of bleeding.
- Recurrent clots: For extended treatment of deep vein thrombosis or pulmonary embolism, DOACs lower recurrence by 34%.
- Death rate: DOAC users have a 10% lower risk of dying from any cause than warfarin users.
But here’s the catch: these benefits shrink if you have poor kidney function. For patients with eGFR under 60, DOACs start to show higher bleeding risks than warfarin. And if you’re under 50 or weigh less than 60 kg? You benefit more from DOACs-especially in preventing major bleeding.
One study in Blood Advances (2022) found that cancer patients on apixaban had 42% less bleeding than those on warfarin. Rivaroxaban? No real advantage. That’s why doctors don’t treat all DOACs the same.
Real-Life Trade-Offs: Cost, Convenience, and Compliance
Here’s where it gets personal.
Warfarin costs $4.27 for a 30-day supply. Apixaban? $587. Rivaroxaban? $523. Even with insurance, your copay might be $50 or $100. For many, that’s a dealbreaker. But here’s the twist: even if you can afford DOACs, you might not take them right.
Studies show DOAC users have 32% higher adherence than warfarin users. Why? Because they don’t need weekly blood draws. No one forgets to take a pill because they’re busy. But forgetting one DOAC dose? That’s risky. Unlike warfarin, which builds up over days, DOACs clear out fast. Miss a dose? Your protection drops fast.
On patient forums, 89% said they prefer DOACs because of no dietary restrictions. 82% cited fewer doctor visits. But 63% of mechanical valve patients still say warfarin gives them peace of mind. Why? Because they’ve been on it for years. They know their body’s rhythm.
Who Should Stay on Warfarin?
DOACs aren’t for everyone. Here’s when warfarin is still the best-or only-choice:
- Patients with mechanical heart valves
- Those with severe kidney failure (eGFR below 15)
- People with advanced mitral stenosis
- Patients with antiphospholipid syndrome (high clotting risk)
- Those who’ve had a clot while on a DOAC
And if you’ve been stable on warfarin for years-with good INR control and no major bleeds-switching might not be worth the risk. Stability matters more than theory.
What About Kidney Patients?
This is a gray zone. For most people with moderate kidney disease (eGFR 30-59), DOACs are still safer than warfarin. But for those with advanced CKD (eGFR under 30) or on dialysis? The data is thin.
The 2023 KDIGO guidelines say: avoid DOACs in dialysis patients unless there’s no alternative. But a 2023 study in Clinical Kidney Journal found DOACs reduced bleeding by 29% in this group compared to warfarin. So what’s the answer? It depends. Some doctors use half-dose apixaban. Others stick with warfarin. It’s a judgment call.
What’s Next?
Researchers aren’t done. A new drug called Librexia™-a combo of warfarin and vitamin K-is in phase 3 trials. It could stabilize INR without daily testing. And the AUGUSTUS-CKD trial, expected in late 2024, will compare apixaban and warfarin in patients with advanced kidney disease and atrial fibrillation.
Market analysts predict DOACs will make up 85% of prescriptions by 2028. But warfarin won’t disappear. It’s too cheap, too well-understood, and too necessary for certain patients.
Key Takeaways
- DOACs are safer than warfarin for most people-with fewer brain bleeds, fewer clots, and less death.
- Warfarin is still the only option for mechanical heart valves and severe kidney failure.
- DOACs don’t need blood tests, but they require perfect adherence-miss a dose, and you’re unprotected.
- Cost is a major barrier: DOACs cost 100x more than warfarin.
- Not all DOACs are equal: apixaban has the best safety profile; dabigatran is best for clot prevention.
Are DOACs safer than warfarin?
Yes, for most people. DOACs reduce the risk of major bleeding by 28% and brain bleeds by 50% compared to warfarin. They also lower the risk of stroke and death. However, they’re not safer for everyone-especially those with severe kidney disease or mechanical heart valves.
Can I switch from warfarin to a DOAC?
Maybe. If you don’t have a mechanical valve, severe kidney disease, or antiphospholipid syndrome, switching is often recommended. But if your INR has been stable for years, your doctor might advise staying on warfarin. Never switch without medical supervision.
What happens if I miss a dose of a DOAC?
DOACs leave your system quickly. If you miss a dose, take it as soon as you remember-if it’s within 12 hours of your usual time. If it’s more than 12 hours late, skip the missed dose and take your next one at the regular time. Never double up. Missing doses increases your stroke risk.
Do I need to avoid certain foods with DOACs?
No. Unlike warfarin, DOACs aren’t affected by vitamin K-rich foods like leafy greens. You can eat spinach, broccoli, or kale without worrying. Alcohol and some antibiotics still matter, but dietary restrictions are minimal.
Which DOAC is safest?
Apixaban (Eliquis®) has the lowest risk of major bleeding among DOACs, based on multiple studies. Dabigatran (Pradaxa®) is best at preventing recurrent clots. Rivaroxaban has a higher bleeding risk, especially in older or frail patients. Your doctor picks based on your kidney function, age, weight, and other meds.
Can I reverse a DOAC overdose?
Yes, but only for some. Andexanet alfa reverses apixaban and rivaroxaban. Idarucizumab reverses dabigatran. Edoxaban has no approved reversal agent. In emergencies, hospitals use activated charcoal, dialysis (for dabigatran), or clotting factors. Time matters-act fast.
What to Do Next
If you’re on warfarin and frustrated with blood tests and diet rules, talk to your doctor about switching. If you’re on a DOAC and worried about cost, ask about patient assistance programs-many drugmakers offer them. If you have kidney disease or a mechanical valve, don’t assume DOACs are right for you. Ask for a specialist review.
There’s no one-size-fits-all blood thinner. Your safety depends on matching the drug to your body-not the other way around.




















15 Comments