Imagine your immune system-the very force designed to protect you from invaders-turns its guns on your own liver. That is the reality for people living with autoimmune hepatitis, a chronic condition where the body attacks healthy liver tissue. It is not just a bad case of inflammation; it is a serious disease that can lead to cirrhosis or liver failure if left unchecked. But here is the good news: we have effective treatments. The standard care involves a combination of steroids and a drug called azathioprine. Understanding how these work, what to expect during diagnosis, and how to manage the side effects is the key to staying healthy.
Understanding Autoimmune Hepatitis
Autoimmune hepatitis (AIH) is not new, but our understanding of it has evolved significantly. First described in 1950 as 'lupoid hepatitis' by Dr. James Waldenström, it was later recognized as a distinct entity in the 1960s when doctors noticed patients responded well to immunosuppressive therapy. Today, the European Association for the Study of the Liver (EASL) notes that AIH predominantly affects women, with a ratio of about 4 women for every 1 man. You might see it in children or older adults, but it peaks in two main age groups: the second decade of life (teens and early twenties) and the sixth decade (fifties and sixties).
The numbers are rising. In the 1990s, incidence was low at 1-2 cases per 100,000 people. By 2023, that number jumped to between 2 and 18 per 100,000. This increase suggests better detection or perhaps environmental triggers we are still studying. The goal of treatment is simple: stop the immune attack to prevent scarring (fibrosis) and eventual liver failure.
How Doctors Diagnose Autoimmune Hepatitis
There is no single 'yes or no' test for AIH. Instead, doctors look for a specific pattern across blood tests, antibody profiles, and liver tissue samples. Think of it like solving a puzzle where several pieces must fit together.
Blood Tests and Antibodies
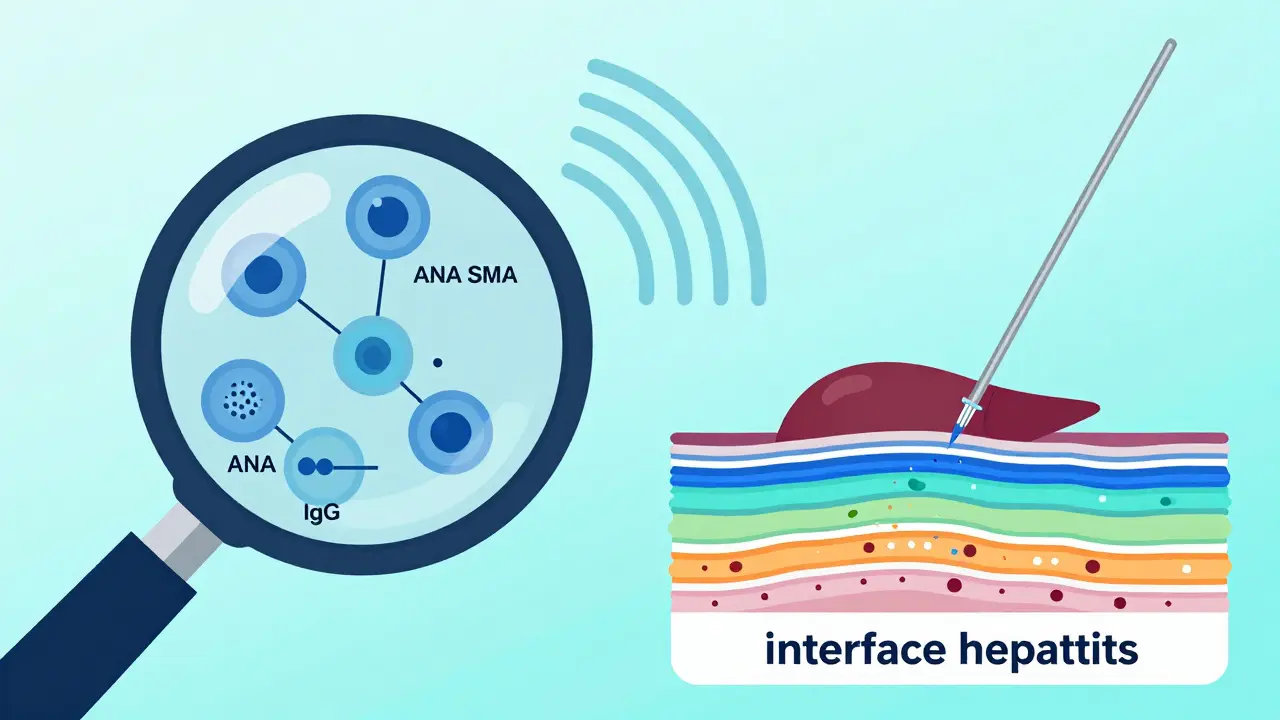
- IgG Levels: Immunoglobulin G (IgG) is an antibody produced by the immune system. In AIH, levels are often elevated to at least 1.5 times the upper limit of normal.
- Autoantibodies: About 80% of cases are Type 1 AIH, marked by antinuclear antibodies (ANA) or smooth muscle antibodies (SMA) at titers of 1:40 or higher. Type 2 AIH, which is rarer and often seen in children, involves liver-kidney microsomal type 1 antibodies (LKM1).
- Liver Enzymes: Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels are usually 5 to 10 times higher than normal during active disease.
The Role of Liver Biopsy
A liver biopsy remains the gold standard for confirmation. Doctors use a thin needle, guided by ultrasound, to take a small sample of liver tissue. They look for 'interface hepatitis,' which is inflammation at the boundary between the portal areas and the liver cells. The 2025 EASL guidelines emphasize that this histological evidence is mandatory for a definitive diagnosis. While there is a small risk of bleeding (0.1-0.3%), the information gained is crucial for tailoring your treatment plan.
| Marker | What It Shows | Typical Finding in AIH |
|---|---|---|
| IgG Levels | Immune activity | >1.5x upper limit of normal |
| ANA / SMA | Type 1 Autoimmunity | Titer ≥1:40 |
| LKM1 | Type 2 Autoimmunity | Present in rare cases |
| Biopsy | Tissue damage | Interface hepatitis |
Steroids: The First Line of Defense
When you start treatment, your doctor will likely prescribe prednisone or prednisolone. These are corticosteroids that powerfully suppress the immune system. Dr. Jay Hoofnagle established this standard regimen at the National Institutes of Health in the 1970s, and it remains effective today.
How It Works
You typically start with a high dose-between 0.5 and 1 mg per kilogram of body weight per day, capped at 60 mg. Within two weeks, most patients (80-90%) see their liver enzymes drop significantly. This rapid response actually helps confirm the diagnosis. Over the next eight weeks, the dose is gradually tapered down to a maintenance level of 10-15 mg daily.
The Side Effects Reality Check
We need to talk about the downsides. Steroids are powerful, but they come with a heavy price tag in terms of side effects. According to patient surveys, many find these side effects worse than the original symptoms. Common issues include:
- Weight Gain: Fluid retention and increased appetite can lead to gaining 30 pounds or more quickly.
- Moon Face: Facial swelling is common and distressing.
- Mood Changes: Insomnia, anxiety, and irritability are frequent complaints.
- Long-term Risks: Prolonged use increases the risk of osteoporosis (20% within 5 years), diabetes (15%), and cataracts (10%).
This is why doctors rarely keep you on steroids alone for long. We want to get you off them as soon as safely possible.
Azathioprine: The Steroid-Sparing Partner
Enter azathioprine (brand names Imuran, Azasan). This drug works differently than steroids. It slows down the production of immune cells that attack the liver. When combined with prednisone, azathioprine allows doctors to reduce the steroid dose by 70-80% within six months. This 'steroid-sparing' effect is critical for minimizing those nasty side effects mentioned above.
Dosing and Monitoring
You usually start azathioprine at a low dose, around 50 mg per day, and slowly increase it to 1-2 mg per kg per day (max 150 mg). It takes time for the drug to build up in your system, so patience is key. Your doctor will monitor your blood counts closely because azathioprine can affect bone marrow function, leading to lower white blood cell counts.
Important Safety Test: TPMT
Before starting azathioprine, you should ask about TPMT testing. Thiopurine S-methyltransferase (TPMT) is an enzyme that helps your body process this drug. About 0.3% of people have a complete deficiency. If you lack this enzyme, azathioprine can cause severe, life-threatening bone marrow suppression. Testing costs $250-$400 in the U.S., but it is a smart investment in safety. The 2025 EASL guidelines strongly recommend this pre-treatment screening.
Treatment Outcomes and Long-Term Management
So, does this treatment work? Yes. About 60-80% of patients achieve a complete biochemical response, meaning their ALT, AST, and IgG levels return to normal within 18-24 months. Even better, recent data shows that treatment can reverse liver fibrosis. One patient reported going from stage F3 (severe scarring) to F0 (no scarring) after two years of therapy.
Relapse Rates
Here is the tricky part: AIH is a lifelong condition for most. If you try to stop medication after achieving remission, there is a 50-90% chance of relapsing. Most relapses happen within three months of stopping. Because of this, 60-80% of patients need long-term maintenance therapy, often at very low doses (e.g., 5mg prednisone + 75mg azathioprine).
What If It Doesn't Work?
About 10-15% of patients do not respond to first-line therapy. In these cases, doctors switch to second-line options like mycophenolate mofetil (CellCept) or calcineurin inhibitors. Newer drugs like obeticholic acid (Ocaliva) are also showing promise in clinical trials, offering hope for refractory cases.
Patient Perspectives and Practical Tips
Reading forums like Reddit’s r/liverdisease gives you a real-world view. Patients describe the struggle of 'moon face' and insomnia but also celebrate victories like normalized lab results. Here are some practical tips from the community and experts:
- Vaccinate Early: Get Hepatitis A and B vaccines before starting immunosuppressants. Once you are on steroids, vaccines are less effective (40-60% efficacy vs. 90% in healthy people).
- Monitor Regularly: Expect blood tests every 2-4 weeks initially, then every 3 months. Don’t skip these appointments.
- Watch for Side Effects: Report any signs of pancreatitis (severe abdominal pain) or unusual bruising immediately. These could signal azathioprine toxicity.
- Join Support Groups: Organizations like the Autoimmune Hepatitis Association provide resources and emotional support. Knowing you aren’t alone helps immensely.
Can autoimmune hepatitis be cured?
Currently, there is no cure for autoimmune hepatitis. However, it can be managed effectively with medication. Many patients achieve long-term remission where liver function returns to normal and inflammation stops. Some may eventually taper off medication under strict medical supervision, but relapse is common.
Why is a liver biopsy necessary if I have positive blood tests?
Blood tests show immune activity, but they don't prove liver damage. A biopsy confirms the presence of interface hepatitis and rules out other liver diseases. It also helps determine the stage of fibrosis, which guides treatment intensity and prognosis.
What are the most common side effects of azathioprine?
Common side effects include nausea, fatigue, and increased susceptibility to infections. More serious but rarer risks include bone marrow suppression (low blood counts) and pancreatitis. Regular blood monitoring helps catch these issues early.
How long does it take for steroids to work?
Most patients see a significant drop in liver enzymes within 2 weeks of starting prednisone. This rapid response is a key diagnostic feature of autoimmune hepatitis. Full normalization of labs may take several months.
Is TPMT testing really necessary before starting azathioprine?
Yes, highly recommended. TPMT testing identifies individuals with a genetic inability to metabolize azathioprine safely. Without this test, deficient patients face a 30-fold higher risk of severe, potentially fatal bone marrow toxicity.